Inflammatory bowel disease (IBD) refers to two related but different diseases: ulcerative colitis and Crohn's disease. These diseases cause chronic inflammation of the intestinal tract, which leads to a variety of symptoms. The inflammation can also lead to involvement of organs other than the intestines. IBD is a lifelong disease with periods of active disease alternating with periods of disease control (remission). IBD is sometimes confused with but is different than irritable bowel syndrome.
There are more than 1 million people with IBD in the United States with new cases diagnosed at a rate of 10 cases per 100,000 people. These diseases account for 700,000 physician visits per year and 100,000 hospitalizations per year in the United States. Ulcerative colitis can be cured with surgery but Crohn's disease cannot be cured. There are good medical therapies available for both diseases.
IBD is generally a disease of young people because it most commonly develops between the ages of 10 and 30. However, a second smaller peak of developing IBD is seen between ages of 50 and 60.
There are racial and ethnic differences in the risk for developing IBD. Whites have a higher risk of developing IBD than non-whites. Similarly persons of Jewish ethnic background have a higher risk of developing IBD than those of non-Jewish background. In addition, among persons of Jewish ethnic background, the risk of IBD is higher for those of Ashkenazi Jewish descent compared to those of Sephardic Jewish descent.
The exact cause of IBD is not known but is related to protective immune cells that are present in the lining of the intestines. This immune system normally turns on and off to fight harmful substances like bacteria and viruses that pass through intestines. In IBD it appears that there is an initial trigger such as an infection or something taken in from the diet or the surrounding environmental that activates the immune system. However, the difference in those who develop IBD is that the immune system does not turn off once this initial trigger is eliminated. This leads to uncontrolled inflammation and attack on normal intestinal cells. The exact contributions of such factors are poorly understood and are difficult to define.
The best-documented environmental factor associated with IBD is cigarette smoking. Smokers are more likely to develop Crohn's disease than non-smokers. In addition, among those with Crohn's disease, smokers tend to have a more aggressive form of disease than non-smokers. Interestingly, the opposite is true for ulcerative colitis, that is, smokers are less likely to develop ulcerative colitis and tend to have a less severe course than non-smokers. The exact effects of cigarette smoking on the intestinal tract and risk for IBD are not well understood.
Finally, there is a genetic (hereditary) risk of developing IBD: 10-20% of IBD patients have one or more other family members affected with IBD. The occurrence of Crohn's disease is increased among relatives of Crohn's disease patients while the occurrence of ulcerative colitis is increased among relatives of ulcerative colitis patients. Both diseases can also exist in the same family with one family member having ulcerative colitis and another family member having Crohn's disease.
In ulcerative colitis, inflammation occurs only in the large intestine (colon) and is limited to the inner lining of the intestinal wall. The inflammation nearly always starts in the lowest part of the colon (the rectum) and extends upwards in continuous pattern. The length of colon that is involved varies between patients. In some patients, the inflammation is confined to the rectum only, in others it extends part of the way up the colon, and in others it involves the entire colon. Because the inflammation is confined to the colon, ulcerative colitis is curable by surgical removal of the colon. Crohn's disease, on the other hand, can involve any part of the intestinal tract from the mouth to the anal area. The most commonly involved areas are the lower part of the small intestine (the ileum) and the colon. Unlike ulcerative colitis, "skip" lesions can be found in Crohn's disease- this means that there can be normal areas in between areas that are inflamed. In addition all layers of the intestinal wall can be involved which may lead to particular complications that are seen only in Crohn's disease including: 1. fistula- an abnormal connection between the intestine and other organs, 2. abscess- collection of pus, 3. stricture- an area of narrowing that can lead to intestinal blockage. Because Crohn's disease usually comes back after surgery, it is generally not curable.
The most common symptoms seen in both ulcerative colitis and Crohn's disease are diarrhea, rectal bleeding, urgency to have bowel movements, abdominal cramps and pain, fever, and weight loss. In Crohn's disease, symptoms can result from complications of the disease. Fistulas can lead to openings in the skin and around the anal region that drain stool and infected material. An abscess can lead to symptoms of severe pain and fever. A stricture can lead to intestinal blockage with symptoms of filling up quickly after meals, nausea and vomiting.
In addition, organs other than the intestinal tract can be involved by the underlying inflammation of IBD. These organs include the eyes (symptoms of red eye or blurred vision), the mouth (symptoms of sores in the mouth), joints (symptoms of joint pain with or without joint swelling and redness), and skin (symptoms of rashes or skin ulcers most commonly involving the lower legs).
The initial part of the evaluation of a patient with the above symptoms includes a full medical history and physical examination. Doctors collect information such as the details and duration of symptoms, whether there is a family history of IBD, and cigarette smoking history. Blood tests can help detect changes such as low red blood cell counts (anemia), high white blood cell counts (indicate inflammation or infection), and low nutrient levels. Stool samples are sometimes checked to rule out intestinal infections, which can lead to similar symptoms as those of IBD.
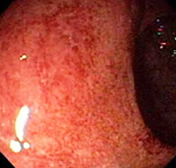
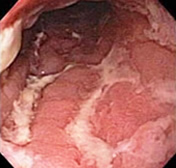
The most direct way to make a firm diagnosis of IBD involves the use of endoscopy (putting a tube with a light at the end into the intestines), biopsies, or special X-rays. With endoscopy, the lining of the intestinal tract can be directly seen by the doctor performing the procedure and biopsies can be obtained. Typical changes of IBD can be detected by endoscopy and by examining biopsies under a microscope. Picture 1 shows the appearance of a normal colon at endoscopy while Picture 2 shows an inflamed colon that is typical for the appearance of ulcerative colitis at endoscopy. Picture 3 shows ulcers in the intestine that are typical for Crohn's disease. Barium X-rays known as small bowel series are also commonly used to diagnose IBD. Patients drink barium (a white fluid), which allows doctors to take X-ray pictures of the small intestine and to look for changes typical of IBD. This test is particularly helpful in evaluating the small intestine, which is the part of the intestinal tract that cannot be fully examined with endoscopes. Another type of X-ray that is sometimes done in patients with IBD is a CAT scan, which is used to look for the presence of an abscess in the abdomen of patients with Crohn's disease. Capsule endoscopy is a newer test in which a pill is swallowed and then travels through the small intestine taking pictures that are transmitted to a recorder and later viewed on a computer. Recent studies indicate that capsule endoscopy is more sensitive for Crohn's in the small intestine than x-rays, but the role of capsule endoscopy in Crohn's disease is not yet identified.
Because ulcerative colitis and Crohn's disease are chronic illnesses, they often require long-term treatment with medications. In general there are two main goals of medical therapy for IBD: 1. Bring active disease under control (into remission), and 2. Keep the disease in remission. Fortunately, there are several good medical therapies available to treat IBD and the most commonly used drugs will be reviewed below.
Aminosalicylates:
These types of medications are among the most commonly used to treat IBD and include agents such as sulfasalazine (Azulfidine®) and mesalamine (Asacol®, Pentasa®, Colazal®). The active component of these medications is a compound named 5-aminosalicylic acid, which works to reduce inflammation in the intestinal wall. These compounds are prepared differently and based on this release 5-aminosalicylic acid in different parts of the intestinal tract. All the above preparations come as pills taken by mouth but there are also suppository and enema forms of mesalamine that are applied directly into the rectum and used to treat patients with inflammation in the bottom part of the colon.
These medications work well for mild to moderate ulcerative colitis and Crohn's disease affecting the colon. They are not as effective for Crohn's inflammation of the small intestine or for more severe IBD. When effective, they work both to bring active disease under control and to maintain disease in remission. They are generally well tolerated with minimal side effects.
Steroids:
Steroids such as prednisone and methylprednisolone are commonly used to treat patients with both ulcerative colitis and Crohn's disease. These particular types of steroids are called glucocorticoids and work as anti-inflammatory agents. They are different from anabolic steroids, which are known for their use by body builders and athletes.
The main role of these medications in IBD is to bring the disease into remission. For patients whose disease seems to require repeated or chronic steroid courses, other medical treatment options described below are available and should be pursued (see discussion of side effects below). Most commonly these medications are given orally. However, in moderate to severe cases of IBD, patients are brought into the hospital and intravenous steroids are used to bring the disease under control. There are also enema and suppository preparations of steroids available.
There are multiple possible side effects from steroids most of which are more likely to develop with higher doses and longer duration of therapy. Early side effects can include mood changes, irritability, difficulty sleeping, increased appetite, and increased blood sugar levels. Side effects associated with long-term use include osteoporosis (weakening of the bones), cataracts, acne, development of a fatty hump at the base of the neck, and a rounded/swollen appearance to the face (moon facies). Although there are possible side effects from these types of steroids, they remain an important part of the medical management of inflammatory bowel disease. With appropriate dosing and tapering regimens, most patients tolerate steroids well.
More recently a new steroid preparation named budesonide (Entocort®) has been made available in the United States for treatment of Crohn's disease. This steroid is specifically designed to release in the intestines with very little of it reaching the bloodstream. Because of this, budesonide has less in terms of side effects when compared to conventional steroids. In its current formulation, this agent works mostly in treating inflammation in the bottom part of the small intestine (the ileum) and the right part of the colon.
Mercaptopurine and Azathioprine:
6-mercaptopurine (Purinethol®) and azathioprine (Imuran®) work to decrease the activity of the immune system, which then leads to reduced inflammation in the intestines. They are used both in ulcerative colitis and Crohn's disease to bring active disease under control and to maintain disease in remission. They are given orally as pills.
These agents may take a few weeks to months to take their full effect, so other medications such as steroids are sometimes needed on a short-term basis to keep disease under control when starting 6-mercaptopurine or azathioprine. These medications have less long-term side effects than steroids. Approximately 5-10% of patients cannot tolerate these medications due to side effects such as allergic reactions, pancreatitis (inflammation of the pancreas), and abnormal liver tests. Because these medications affect the immune system, patients have a higher risk of developing infections. Therefore, it is recommended that blood counts be monitored on a frequent and regular basis when on these medications.
Methotrexate:
Methotrexate is another medication that works to decrease the activity of the immune system. It is used in Crohn's disease both to bring disease into remission and to maintain remission. There have been some reports of methotrexate for treatment of ulcerative colitis but there are no controlled studies that have shown a benefit. Methotrexate can be given either as pills or as an injection under the skin or into the muscle, but the studies that have shown that it works in IBD have used the injection approach. A vitamin named folate (or folic acid) should be given with methotrexate to decrease some of the side effects. Potential side effects and risks include nausea, vomiting, infections, bone marrow suppression, liver inflammation, and rarely scarring in the lungs. Methotrexate is also known to cause birth defects and therefore should not be used in either males or females who are trying to have a baby.
Infliximab:
Infliximab (Remicade®) may be used in moderate to severe Crohn's disease. It is a medication that is given intravenously and works on reducing intestinal inflammation by blocking a part of the immune system know as TNF (tumor necrosis factor). A single infusion or a short series of three infusions have been shown to bring inflammation into remission and to allow closure of fistulas. The benefit may last approximately two months. However, recent studies have shown that repeated infusions of infliximab over a one-year period are generally well tolerated and can maintain remission. Side effects of this agent include infusion reactions, which are usually mild, and infections. Occasionally the infections are quite serious.
For ulcerative colitis, there are two main indications for surgery: 1. Lack of response or intolerance to medications, and 2. Precancerous or cancerous changes in the colon. Patients with ulcerative colitis have a higher risk of developing colon cancer so careful monitoring of the colon by colonoscopy is recommended in those who have had the disease for many years. As previously discussed, surgery allows for a cure in ulcerative colitis. However, removal of the colon used to mean that patients would have to have a permanent stoma (wearing an external bag to drain stool). Currently, a procedure known as the pouch procedure can be done in most patients with ulcerative colitis and this prevents the need for a permanent stoma. In this type of surgery, the colon is removed, a reservoir is created out of the lower part of the small intestine (the ileum), and the reservoir is connected to the anal region.
For Crohn's disease, indications for surgery include lack of response or intolerance to medications and complications of Crohn's such as a fistula, an abscess, or a stricture. Up to 70% of patients with Crohn's disease require surgery at some point in the course of their disease. The risk of having Crohn's disease return after surgery is approximately 70-85% within 10-15 years after surgery. There is growing evidence that medications can be used to decrease the risk of Crohn's returning following surgery.